Shoe Research Project Gävle
Compiled in cooperation with The
Department of Family Medicine,
University of Uppsala, Sweden.
Summary
Goal: to show that a method for shoe and foot
analysis developed with the help of two swedish athletic stores, including foot and shoe classification, video-filming
of walking or running on a treadmill, and individually fitted shoes,
1) decreases pain/problems with ordinary
exercisers and
2) indicates that the current practice of
prescribing orthotics to many joggers/exercisers is often quite unnecessary.
Method: Testing of the participants of this study was
performed by two shoe salesmen, who had no previous medical education, and an
orthopedic engineer. Patients/subjects were randomly distributed among their
regular customers. The salesmen received a two day course in shoe and foot
analysis prior to this study. This education was given by the orthopedic
engineer and a physician, both with several years of experience in this method
and of shoe classification.
The treatment group (T) consisted of 86
randomly selected patients complaining of problems/pain during jogging or
walking. Group (T) received
individually fitted shoes from the onset, while a control group (C) received
individually fitted shoes after a 3 month period. Follow-up studies were made
after 3, 6 and 36 months.
Only shoes from the standard assortment of the
athletic stores were used. (No specially-designed shoes were included.) The
subjects of this study were aged 12 - 78 years, with middle-aged individuals
predominating. Although not included in this research, earlier experience with
the above method revealed that even younger children can benefit from these
same techniques.
History of ailments: 55% of the patients in this study had
experienced problems for 5 years or more. 35% had experienced problems for more
than 10 years. Only 10% had experienced problems for less than one year. The
problems treated originated in the feet, the Achilles tendon, the lower leg,
knees and hips, but improvements were even noted in patients complaining of
problems in the lower back.
Results - after 6 months: In group (T), more than 50% of all
participants were completely free of discomfort. One person was problem-free
after having experienced walking pains since the 2nd World War! Out
of the 40-50% remaining who were not
completely freed of discomfort, their problems decreased by appox. 60%. Only 4
patients reported the same amount of pain following the 6-month period.
Group(C)’s problems remained unchanged during
the first 3 months when properly fitted shoes were introduced.following 3
months, resulting in an immediate reduction in discomfort.
Results – after 3 years: After 3 years 41% of all
participants experienced no pain/problems during exercise, walking or jogging. 56%
were free of pain when not exercising. Apprx 75% of all problems in the feet,
lower legs and lumbar region were cured. 86% of all subjects with knee -pain
experienced no pain at rest, 60% were cured of all knee pain even during jogging.
Only two patients received individually-fitted orthotics after other
fundamental corrections failed to reduce pain or whatever discomfort they
experienced.
The results of this study show that exact
measurement of the foot angles during VCR filming is unnecessary except in special
cases. The most important procedure during the video analysis is to see to that
the foot is somewhat straight and to avoid overcorrection, in particular the
so-called pronation/eversion angles, which is the most usual position of the
foot during the weight-bearing midphase of the step.
When choosing new walking or jogging shoes we
recommend first and foremost that the stability of the shoes are checked
followed by matching the foot-type to the type of shoe selected. The
shock-absorbing abilities of modern medium and high priced jogging shoes are
most often satisfactory. The regular customer need not worry about
shock-absorption unless he/she is extremcly over- or underweight ,or, if
running under extreme conditions is planned.
The results of this study show that a
professional cooperation between shoe salesmen, an orthopedic engineer and a
physician interested in foot and shoe analysis, will produce excellent results
for many patients/customers who have suffered for years or even decades from
discomfort during exercise. The study also shows that patients with problems of
the lower leg, when provided with an adequate choice of shoes, no longer need
rest indicated. Indeed, it is highly probable that many discomforts exercisers
complain of are actually caused by an inadequate choice of shoes. The study
shows that shoe and foot analysis followed by individually -fitted shoes
prevents and results in less pain/problems for ordinary exercisers.
2
Shoe Research Project Gävle
Compiled in cooperation with
The Department of Family Medicine,
University of Uppsala,
Sweden.
Goals
To test the efficacy of a regimen consisting of
shoe and foot analysis including a simple classification of the feet and
running style, followed by correctly fitting shoes in accordance with the
principles of shoe classification as developed at two different athletics
stores in the cities of Gävle and Sandviken, Sweden. This study is meant as a
quality assurance of the already indoctrinated work and analysis routines that
have been in use in these stores for the past several years, a method that
continues to be developed in cooperation with an orthopedic engineer and a
physician.
Method
Following an advertisement in the local paper
during the spring of 1995, where we stated that we were looking for ordinary
exercisers (not professional atheletes) with problems while running or walking,
86 subjects were enlisted, 39 men and 47 women, randomly divided into two
groups.
Treatment Group (T), 46 participants, received
newly-fitted shoes from the onset, while Control Group (C), numbering 40
participants, received shoes after approx. 3 months.
Follow-ups on both groups were performed after
1, 3 and 6 months as well as a 4 month
follow-up for Group (C), one month after they had been issued fitted-shoes.
The final follow-up was performed after 3
years, during the fall of 1998.
The subjects in the Group (C) were free to use
or exercise in their old shoes (or any shoes they preferred) for the 3 months
prior to being analysed and fitted, to assure that their problems did not
disappear by themselves. ”Exercise” in this study was defined as either walking
or runnning for the sake of exercise, to increase or maintain one’s physical
stamina.
The testing of the shoes and video filming the
walking and running steps, was performed by two shoe salesmen (who had no
medical education), together with an orthopedic engineer. Prior to the study
the shoe salesmen received a 2-3 day course in shoe-analysis, running-analysis
and video technology, conducted by the orthopedic engineer and the physician. Both
shoe salesmen had long experience in
shoe-analysis and both had been active
in the shoe-analysis program which had laid the groundwork for the
shoe-classification system used in this study in the above-mentioned stores. Both
salesmen were thoroughly acquinted with the shoe assortment and their
characteristics.
The 6-month follow-up was performed in the fall
of 1995 by a independant physician who had not previously participated in the
selection of any shoes nor in any of the subject’s previous follow-ups. A
medical examination was not performed at this time, because the aim of the
study was to show that the shoe and foot analysis and the shoe-classification
system together with the analytical process currently in use in the
participating stores succeeds in reducing pain for exercisers.
A record of the each of the subjects’ problems
was based on questionnaires and pain-drawings which the subjects were asked to
fill-in at all follow-ups.
The shoes used in this study were of different
brands and had been chosen from the standard athletic store assortment. None of
the shoes were valued at more than 120 USD; most were valued at 50-100 USD. During
shoe selection the subjects were asked for a 50 USD deposit, refundable after
the 6 month period.
Participants
Age spread, duration of problems, and estimated
levels of pain were quite similar in both groups. Distribution of gender was
randomly uneven, 59% males in the Group (T) and 70% females in the Group (C),
for totally 39 males and 47 females. Gender did not appear to have any effect
on the study’s final results. All 86 subjects completed the study through to
the 6th month follow-up. A total of 11 out of the 86 subjects did not
participate in the 3 year follow-up:
6 refused to attend due to unrelated medical
problems or change of address (two developed cancer, one was post-surgery /
disease unrelated to this study, and 3 had moved away),
an additional 5 subjects we were unable to be
contacted.
Not included among the 86 participants in this
study were:
one subject dismissed from the study due to a
general illness which prevented exercise / usage of the shoes he was issued,
and one subject disqualified from the study due to severe arthritis of the foot
joints.
Most of the participants of the project were
middle-aged with 38% between 40-49 years.
Age-spread of the 86 subjects was 12 - 78 years
.
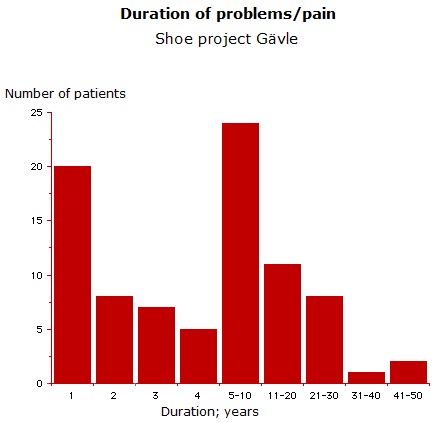
Duration of problems
Participants selected had long-standing
complaints / pain, averaging approx. 8 years.
Only 10% had suffered for less than one year,
while 55% had a history of discomfort spanning 5 years or more. Approx 35% had
experienced problems for more than 10 years. All were equally divided between
Groups (C) and (T).
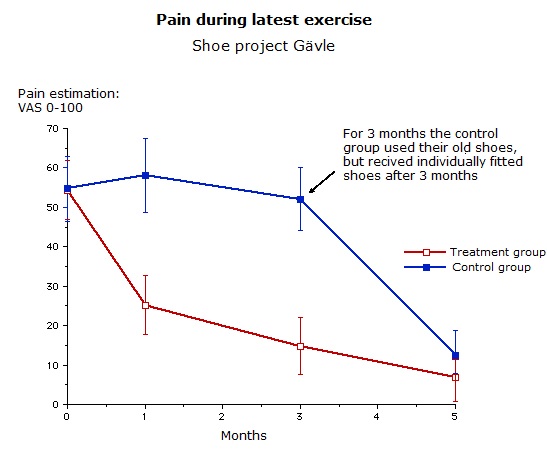
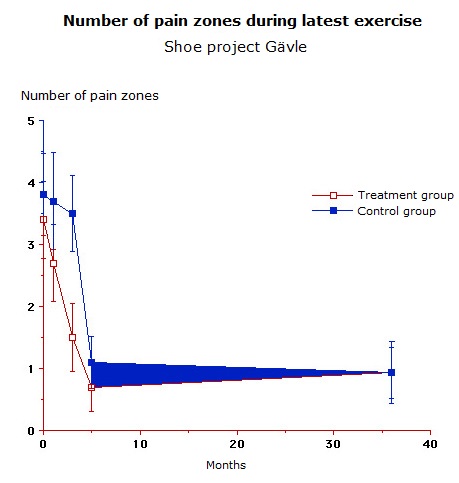
6 month results
The problems continued unchanged with Control
Group(C)’s subjects (who had been free to exercise in their old shoes or shoes
of their own choice), until after the 3-month period. Upon receiving their new
fitted-shoes, their problems reduced dramatically in the same manner as for
Treatment Group(T) (who had received fitted-shoes at the onset of the study).
82 of the 86 participants felt an improvement
of their problems. 61% of Group(T) and
45% of Group(C) were totally cured (no remaining problems). The discrepancy is
explained by Group(C)’s 3 month shorter use of the shoes vs Group (T).Our
expectations of a further decrease in Group(C) levels of discomfort to a level
equivalent with Group(T) was vindicated by the results of the 3-year follow-up.
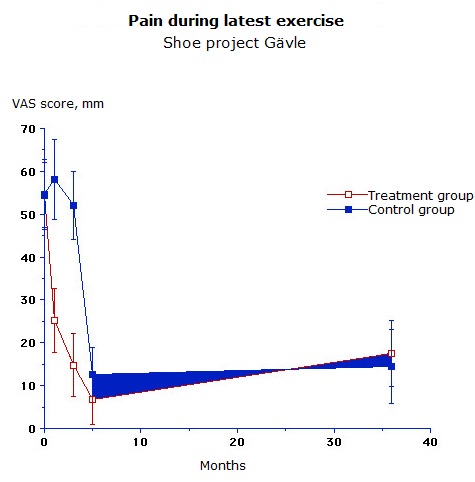
On a pain scale (VAS 0-100) the average value
decreased from 48-55 to a median of approx. 19-20.
Only 4 subjects did not decrease their pain
score. Following a doser analysis it was noted that 3 of these had partially
improved in some of their symptoms, while some symptoms still remained, resulting
in an equally high pain score totally, according to the VAS-method. Only one
subject continued to have the same level of pain score following the 6 month
period as he had experienced at the onset of the study, but he maintained the
same level and intensity of exercise (several full rounds of golf per week).
3 year results
The problems that were treated originated from
the feet, Achilles tendons, lower legs, knees and hips, but problems in the
lower back were also relieved.
Only two subjects received individually-made
orthotics, but only after other fundamental corrections failed to reduce pain
or whatever problems they experienced.
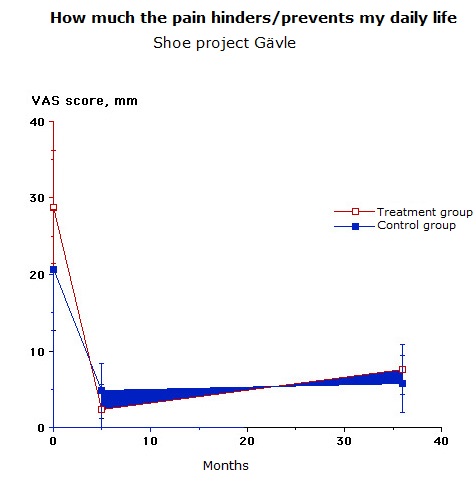
After 3 years 41% of all subjects reported no
pain/problems during exercise, walking, or jogging (no pain in any part of the
body) and 56% were free of pain when not exercising.
Approx 75% of all discomforts in the feet,
lower legs and lumbar region were cured after the first 6 months.
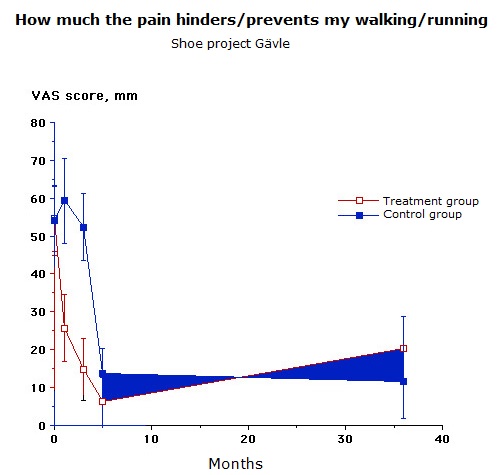
86% of all subjects with knee pain experienced
no pain at rest, while 60% were free from all knee pain even during jogging or
walking. The lowest score in the study occurred with hip discomforts, where
only 40% were relieved.
A slight tendency toward increased pain was
noted at the 3 year follow-up vs the 6-month results. This tendency was not statistically
significant in several of the parameters tested. Those experiencing an increase
in foot discomfort were limited to the Group(T), who had received individually
fitted-shoes directly upon entering the study. Some hip problems also
increased, but these occurred mainly at rest, strangely enough not while
exercising. Those experiencing diminished pain in the knees or lumbar region
after 6 months reported no increase at the 3 year follow-up.
Neck problems were reduced from 12% to 7% and
thoracic pain was reduced from 8% to 3%: no significant conclusions could be
drawn from this, as these problems were in the minority at the onset of the
study.
Especially notable were that knee discomforts
cured faster than foot problems after individually fitted-shoes were worn.
Early on, 2-3 months after the fitted-shoes
were issued, significant relief from knee discomfort took place. This decrease
in knee pain continued through both the 6-month and the 3 year follow-up..
Foot and lower leg pain took somewhat longer to
relieve: useful information when discussing recovery-time with a patient.
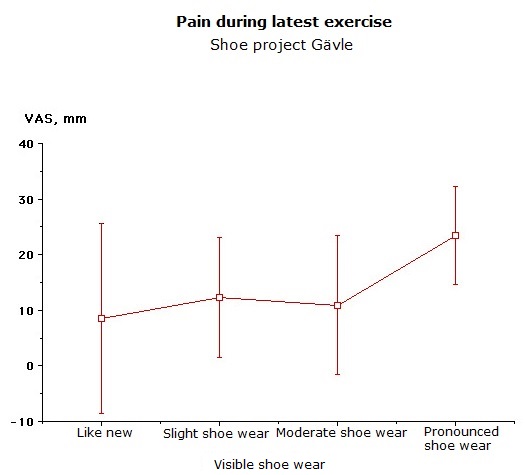
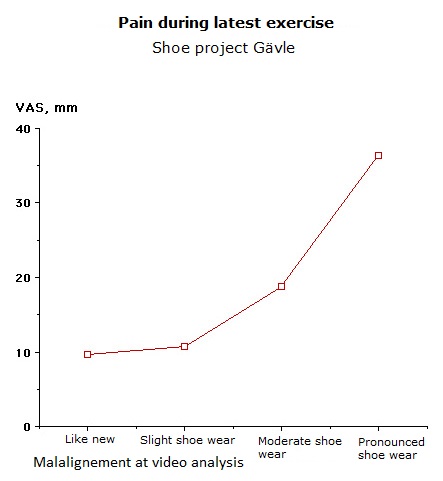
The slight tendancy to experience more
discomfort after 3 years, compared to after 6 months, is statistically and
significantly correlated to the collapse of the material in the shoes: a
collapse evidenced conclusively with slow-motion video. The results of the
study clearly indicate that it is quite difficult for even experienced staff to
visually assertain if shoes are worn out. Only when the shoes displayed severe
wear/damage, was this statistically correlated to increased pain. A perusal of
the outward appearance of the shoes often gave no indication as to their true
condition! Collapse usually occurred long before the shoes began to appear
worn.
Conclusion: significant collapse of the
material could only be detected using slow motion video.
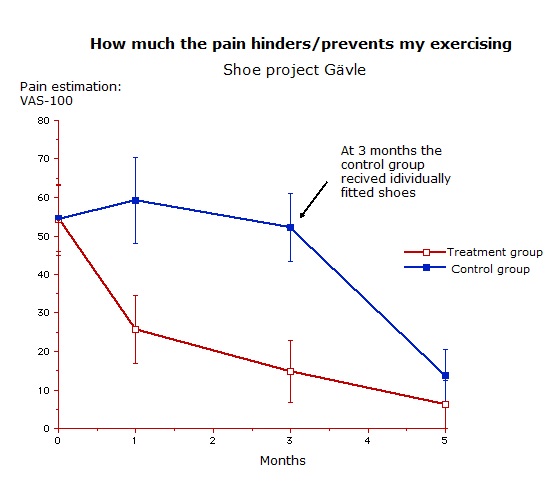
Intensity and frequency of exercise activities
With decreased pain both the intensity and
frequency of exercise increased: test subjects reported being able to exercise
both longer and more often. Activities increased to the 6 month follow-up,
decreasing somewhat by the 3 year follow-up. Both subjects who performed no
exercise whatsoever, and those who normally exercised a good deal, were able to
increase their activities substantially by the 6 month follow-up and maintained
this level to the 3 year follow-up. Those subjects falling in between also
enjoyed increased activity by the 6 month follow-up, albeit somewhat less. This
activity level decreased by the 3 year follow-up for unknown reasons.
ln
Group(C) no increased level of activity was noted until after the 3
month control.
The majority of the subjects in this study were
either unable to exercise, or severely hindered in their activities at the
onset of the study and had been so for long periods of time. The change to
fitted-shoes clearly made it possible for the participants to increase their
activities due to diminished pain. Group(C) did not increase their activities,
experiencing undiminished discomfort, until the time when they received
fitted-shoes.
Comments
This project has proven that the measures taken in this study have not
only a short term, but also a long term effect.
It is important to note that no
special shoes were used for this study, and that only two subjects were given
orthotics (individually molded and fitted inserts). Cheap wedges, anterior arch
supports and simple prefabricated insoles have been complemented where needed.
-Slow-motion
video analysis and freeze-frame techniques together with the treadmill are considered
to be important tools and methods. Of equal, if not greater import, are the
following parameters where the foot-type decide the choice of shoes:
-Correct width of the shoe. The shoe must allow space for the foot
to widen approx. 1/3 inch when pressure is put on the anterior arch of the foot
in the weight-bearing phase of the step.
-Correct length of the shoe. The shoe must allow space for the foot
to elongate approx. 1/3 inch when pressure is put on the longitudinal arch of
the foot in the weight-bearing phase of the step.
-Sufficient anti-torsion characteristics in the sole
-The sole should bend where the
toes bend (approx. 1/3 to 1/4 of
the length of the sole from the front end of the shoe along the
"metatarsal break" = the
axis of movement)
-Insoles should be washable and exchangeable, to give place for wedges, inserts and
orthotics if necessary.
-Sufficient stability of heel cap to hold the foot correctly in place and
to prevent malpositioning of the feet.
-Rounded heel (or other construction with similar effect) for smoother
heel-strike.
-Adjusted toe box (front of the shoe) suited to the
anatomy of the toes and fore foot
-Correct last for the foot type. In general, a flat
foot will need a straight (medial) inner margin of the sole and a high arch
will need a curved sole. Exceptions to this may occur, for example: there is at
times a difficulty in finding wide enough shoe for people with high arches who
normally should be given shoes with a curved sole. In order to fit the foot
into a shoe we sometimes have had to supply customers or patients (also some
participants in this study) with the ideally "wrong" last in order to
initially find a shoe for them with other acceptable characteristics. The
choice available when fitting shoes will at times not be ideal when limited to
the standard assortment of commercially available shoes. Notwithstanding, the
results of this study prove that the simple testing procedures used in this
project work extremely well.
-Finally: Vital are educated
personell with an understanding of what is to be analyzed. A treadmill and
a VCR placed in a store is no guarantee of good results.
Even when orthotics are placed in
the shoes, a video analysis on a treadmill should be performed to check the
results: most orthopedic departments currently lack this essential routine.
Video analysis on a treadmill should
be performed at the same speed normally used walking or running, since
weight-bearing and the angles of the foot will vary with different running or
walking speeds.
Measurment of angle between heel and center of lower leg and the misuse
of the terms ”pronation” and ”supination”
In the past we were all taught to use exact
measurements of the so-called "pronation” and "supination"
angles, filmed from behind, to determine the angle between the Achilles tendon
and the longitudinal length axis in the middle of the lower leg. The practice
is still currently in use, but in our opinion, information obtained by
measuring this angle gives not only incomplete, but also both flawed and conflicting
information.
Measurments of this angle will vary
with differing running speeds. They also vary depending on how familiar the
tested person is with running on a treadmill and the length of time this person
runs during the test. The angle will also vary with the differing measuring
techniques between one shoe salesmen and another.
Of vital importance: this angle also
reflects the degree of bow-leggedness a person has. The foot can be corrected
to a completely straight position but the angle measured will still show
"pronation" due simply to bow-leggedness. It is our experience that
trying to correct this "pronation", although the foot is straight,
will create overcompensation and most surely increased problems for the
customer. For these reasons we have abandoned this technique years ago.
From a medical biomechanical
standpoint, the movements of pronation and supination occur in the forefoot
only, and around a completely
different axis than the heel movements, which occur in the subtalar joints -
termed inversion and eversion. Besides these movements, there is considerable
instability within the ankle (foot joint) itself, which enhances the impression
of in- and eversion of the ankle or heel. This instability increases with more
plantar flexion of the foot. Furthermore, the movements of both the forefoot
and the heel are different in different
stages of the step. Therefore the step should be also analyzed during the other
weight-bearing phases rather than just during the midphase of the step. Focusing
on the heel angle thus becomes less important.
The foot’s outward movements
(pronation/eversion = pes valgus) are more important to study during the mid-
and endphases of the step. The foot's inward movements (supination/inversion =
pes varus) are more important to observe during the heel-strike and mid-phase. Pronation
of the forefoot is more common (approx. 75%) than supination (less than 5% )
and is part of the body’s own shock-absorbing mechanism. A jogger with
supination/inversion will experience his legs as considerably less
shock-absorbing; they will feel stiff while running and he will frequently have
problems in the feet or hips, according our previous experience. On the whole,
our experience shows that supinators have more problems than pronators. Supination
is more difficult to detect and therefore not as easy to treat and correct as
is pronation.
We recommend that in the future a more precise
and correct terminology be used, our
essential argument being that these different movements during a running
analysis need to be strictly differentiated.
We would like to be rid of such terms as
"pronation", "underpronation" and "supination"
regarding the movements of the heel. The term "forefoot pronation" is
unnecessary since pronation only takes place in the forefoot and not in the
heel. The term "(anti)pronation wedge” should be used only for
wedges that correct movements of the forefoot.
Principles of video analysis
Our goal in this study was to find out if the
following simple principles of correcting the foot during video analysis were
enough to cure pain or eliminate experienced problems.
a) In correcting the heel-strike phase at a
moderate running speed it has been our goal to avoid extreme outer positions of
the heel in inversion, to avoid problems of the hip region and the pelvis.
b) During the mid phase of the step both
movements of the heel and forefoot have been corrected, so that the foot stands
seemingly straight without having to correct too much or to care too much about
the exact positioning the foot. In our earlier experience a more exact
correction than this, will in most cases, be unnecessary.
Only if this correction did not produce
satisfactory results, were finer adjustments
performed
In this study we never
measured heel angles exactly.
During the mid-phase of the step we took pains
to avoid overcorrecting someone with pronation/eversion.
c) We corrected subjects with
supination/inversion more carefully. If supination/inversion was evident during
the midphase, the subjects were corrected to a strictly neutral position
The use of orthotics
In this study we have shown that several
problems of the lower extremities can be cured or reduced solely by the use of
individually fitted-shoes. Many people in this study who had experienced problems
for several years and who previously had been examined and treated without much
success by healthcare specialists
(doctors, physiotherapists, orthopedic engineers, acupuncture etc),
experienced a radical improvement or were completely cured.
Often specially fitted orthotics are not
needed. Orthotics have become a livelihood amongst orthopedic engineers and
orthopedic technicians at running-clinics and orthopedic workshops. We consider
that orthotics are an important supplement, but only when one fails to choose
an adequate shoe design.. According to our extensive experience, orthotics are
needed in less than 5% of all shoe store customers. In our study we needed to
supply only 2 out of 86 subjects with them. Others claim that up to 53% need
orthotics (Graversen-Simmons: Previa-Löplabbet, Study on mailmen in Borås and
Gothenburg, Sweden).
Our advice is to always begin with a
well-fitted choice of shoes. To put orthotics into shoes that have not been
analyzed or into shoes that are not fitted to the individual, is by our
standards deficient methodology. We have met several patients who have had
problems for years, who were prescribed specially fitted orthotics and who
still were not rid of their problems. Yet when these shoes and supplements were
discarded for properly fitted-shoes using the simple methods tested and proven
effective in this scientific project, they were freed of discomfort..
Stability
Less stable shoes can be fine to walk or stand
in, although they might prove less useful for running or walking longer
distances. Lighter shoes are often preferred, feeling more comfortable to run
in than heavier ones (ie. for a marathon). For the average exerciser/jogger we
recommend that he regard stability as a first priority, which at times may mean
a slightly heavier shoe.
A lighter, perhaps less stable shoe might
possibly prove faster in a competition, particularly for those who do not weigh
very much, but for basic training we recommend a more stable shoe to prevent
injuries.
Shock-absorption
Shoe producers often make advertising claims
that shock-absorption is an essential reason to choose a certain shoe. In our
opinion, other than in extreme cases, shock-absorption is no longer an
important argument when selecting shoes. No matter how they are constructed,
most shoes on the market have good shock absorption, with the exception of some
very cheap models.
No shoe brand can be said to be best. No specific shoe can be said to be
the best.
In this study we have used different shoes of
different brands, many well-known world wide and available in most countries of
the world. In this report we chose not to mention what brands we have used
because we consider this of less importance. No funds or other means have been
accepted for the cost of this study from any shoe manufacturer. This study used mostly 7 to 9 different shoe models
from the standard assortment of shoes in an athletics store, with complementary
characteristics of our choice. In addition to these more widely-used shoe
models we have used 3 to 4 other models which we considered necessary to hold
in stock for special customers/patients, but although these shoes are not often
sold, they are nevertheless important to have access to. If for some reason
these 7-9 plus 3-4 models were not available, we would most likely be able to
choose equivalent shoes from other brands complementing each others’
characteristics and thus obtain the
same results.
The individual walking or running
style, as well as the foot’s appearance (width, length, foot -type) will be
effected by the last and therefore the choice of shoes will always be very
individual.
A shoe that is considered to be perfect for one
person might be a poor choice for someone else and vice versa.
One specific shoe model might have different
characteristics different years, a rather common occurrence. Shoes of the same
model and brand can even vary in their characteristics during the same season
even though their appearance remains unchanged !
Expensive shoes are not always better than
cheaper ones!
Famous or well-known brands do not guarantee
good quality or even that the shoe will fit you!
It is important to make sure that
the shoe is functional, ie. fits your foot-type and your running or walking
style and that it suits the activity you will be using the shoe for.
Education
Shoe salesmen should be educated to master the
methods that we used in this
project.
The results
that are shown in the study indicate
that more resources and measures must be taken for exercisers and atheletes
before they have to turn to the healthcare system. These methods can also be used with success for
healthcare patients.
The community encourages people to
exercise. It should be just as important that this wide spread athletic
movement should result in as few injuries as possible, something that this
study shows can be attained by simple means combined with knowledge.
The spread of this knowledge would probably spare a lot
of patients/customers/exercisers
considerable suffering and save the community/healthcare system a great deal of
tax money.
Logically the spread of this
information is not only the responsibility of, but also in the interest of
everyone in the shoe and athletics industry, in healthcare and insurance, as
well as the medical industry and the media.
Other comments
Fitted shoes can give positive
results on certain lower back, thoracic, and as well as neck problems: an
effect we noted in our daily work - and in this study. The number of patients
in this project with these kinds of problems were too few to be able to make
statistically significant conclusions, but an obvious tendency for good results
was evident.
The fitted-shoes must be used to achieve any alleviation
of those problems present.
We noticed that some of the
participants at the onset of the study did not use the fitted shoes very often.
Following recommendations to use the shoes, i.e. to participate in the study,
their problems were most often drastically reduced.
This has practical implications.
Although many in this study improved
in a short period of time, it sometimes took about 1-2 months before the
problems disappeared, and at times even longer. For a realistic approach to
rehabilitation, it is important to inform patients/customers about the expected
time for recovery and future levels / intensity of physical exercise.
Recommendations when shoe analysis fails to reduce pain (not shown in
this study)
If the results following
fitted-shoes and foot analysis are inadequate, the patient/customer should be
examined by medical personnel (physician, physiotherapist, orthopedic engineer,
orthopedic technician etc). It is essential that non-medically trained shoe
salesmen do not develop a belief that they can cure everything by using the
methods we have developed. It is also important that shoestores maintain good
relationships with healthcare personnel, especially in regard to those
customers who are not relieved by shoe corrections.
ln this study we have tested jogging and
exercise shoes from the standard assortment common to most athletics stores. In
our experience, these shoes are also acceptible for walking, for work, and are
often excellent for diabetics and for quite a number of those with foot
deformities. In our opinion these shoes are often better than expensive
specially constructed shoes from orthopedic departments. Indoor shoes and
special shoes for different sporting events have not been tested in this study.
Our recommendations to health care
personnel regarding their patients are: initially, the patient should look in
the athletics / regular shoe stores in town for shoes that will properly fit
him, before being prescribed expensive handmade shoes from the orthopedic
departments.
If shoes from the orthopedic
department do not solve the patient’s problem, the patient should return once
again to search the regular shoestores for shoes that conform to the
recommendations we have outlined in this study.
Conclusions
-By this prospective, randomized
study including a control group, we have shown that joggers and exercisers,
most with a history of leg problems spanning several years (foot, lower leg,
knee and hip), achieved a total improvement in approx. 80% of their problems
(shown in pain evaluation scales) only after being issued fitted-shoes.
-More than half of all of the
participants at the 6 month follow-up and more than 40% after the 3 year results were pain-free. Those who were not
completely cured by this simple method of shoe-fitting, experienced 60% average
reduction in pain. About 75% of the problems in the foot, lower leg and lumbar
region were cured and 60% of all knee problems disappeared: the result of
following a basic analysis and classification method of foot and shoe-type
combined with a simple and fast video analysis of stability with the help of a treadmill.
-We have shown that shoe salesmen without
medical training can be taught this specific method and analysis to the benefit
of the customer/patient
-We have shown that recommending / prescribing
orthotics should not be the first step in finding a solution to walking or
jogging problems.
-The store owner in this study found that
selling shoes using this method saved his staff both time and energy. The
stores also experienced considerably fewer complaints / product returns
and a notable increase in the
quantities of shoes sold after the introduction of this method.
During this study and the development of these
methods we have also learned which characteristics are required for good shoes.
Shoe designs to meet the customers’ needs are often held as a manufacturer’s
secret. This project revealed that many manufacturers are, in effect, unaware
that some of their products on the
market actually cause problems.
Fashion aspects have not at all been considered
in this project, though in our opinion it is perfectly possible to produce
fashionable shoes with good functional characteristics that will prevent pain,
overstraining and other, related problems.
This study was performed by:
Bemt Ersson M.D. Gävle, Sweden
Lasse Höglund, Orthopedic engineer, Gävle
Eje Bergström, Store owner with additional
staff, Intersport Gävle
Kurt Svärdsudd,
Professor, Dept. Family
Medicine, University of Uppsala, Sweden
If you have any questions please feel free to
contact:
Dr Bernt Ersson Strömsbrov. 56 S-806
45 GÄVLE - SWEDEN
Web site: www.shoedoc.se email: bernt@shoedoc.se
fax: + 46(0)26510914 (from abroad) fax: 026-510914 (from Sweden)
office telephone: +46(0)26127600 fr abroad work telephone: 026-127600 from
Sweden
Special comments on Achilles tendon problems
Control Group
ln the Control Group that received
the fitted-shoes and wedges following approx. 3 months, we discovered 10
subjects with Achilles tendon problems.
6 of these were completely cured
with corrections, 2 reported major improvement, while 2 felt no
improvement in their Achilles tendons, in spite of feeling improvements re
other problems they suffered from.
Another 4 subjects in the Control
Group marked calfpain but Achilles tendons pain on their pain drawings. 2 of
these were cured, the other 2 considerably improved.
Everyone in the Control Group had
more than a 1-year history of Achilles tendon or calf problems (excepting 3 who
had experienced problems for only 3-6 months prior). 7 had more than a 12 year
history of problems.
The entire Control Group reported no
change in discomfort during the 3 months before they were issued fitted-shoes. All
improvement occurred within 2 months of
being fitted shoes.
Treatment Group
In this group there were 13 persons
with Achilles tendon problems and l person with calf problems. 10 were
completely cured and another 4 noticed marked improvement.
The improvement occurred relatively
soon after receiving the fitted shoes, mostly within 1-3 months.
7 subjects had experienced problems
for more than 3 years and 4 of them for more than 7 years.
2
subjects had experienced pain for less than l year (2 months and 6
months resp)
Method of correction
It is important to point out in this
situation that after several years of treating athletic injuries and via
research projects, we have noted that problems of the Achilles tendons should
not only be treated by elevating the heel in the shoe with traditional wedges.
It is important to make sure that
the foot during the running or walking step does not have an improper angle,
both in the forefoot (pronation/supination) but also in the rear portion of the
foot (inversion/eversion). Shock absorption of the heel, especially if too
soft, stability of the heel cap and its’ formation, along with the stiffness of
the sole in the front portion of the shoe can be part of the problem.
Conclusion
Although the number of experimental persons
with problems of the Achilles tendon and calf seems low (28 people), our study
indicates a certain strong tendency: Achilles tendon and calf problems can most
definitely be improved with well-fitted shoes, and, if necessary, cheap
supplements of different kinds like wedges and inserts.
If one also considers that most of
the participants of this study had experienced their problems for a long time
(years), and that 26 out of 28 participants were cured or experienced a major
improvement of their problems following correctional adjustments of their shoes
only. This fact, and the fact that the subjects in this study could continue
with their exercising can only lead us
to conclude that rest as a treatment for Achilles tendon problems may not be
the only valid method to prescribe.
Contrary to common practice, we
consider it important to give the patient a well-adjusted choice of shoes along
with a rehabilitation plan including individual instruction on how to train,
including walking, stretching and so-called excentric exercise(recommended) as
opposed to concentric (not recommended).
Inflammation of the Achilles tendon
is considered to be an overstrain injury.
For several reasons it is both debatable and even questionable to
prescribe only rest as a cure for
overstrain injuries.
Oct 2001
Bernt Ersson M.D.
Ideal characteristics of the golf shoe
The ideal golf shoe will be a compromise
between the best characteristics of a walking or jogging shoe and those
necessary for a stable golf swing. Common construction faults of golf shoes are
poor shoe adjustments to the anatomy of the foot (wrong last, width, length,
toe box etc) as well as insufficient stability, poor anti-torsion
characteristics, unstable heel cup and failure to correct foot position while
walking and well in the swing. The heels of golf shoes are often too hard and
thin, the soles too thin and they often bend incorrectly.
-If walking is the option on the
golf course, golf shoes should have most characteristies of good walking shoes
as described in "Shoe Project Gävle". Priorities should be comfort,
stability, anti-torsion characteristics and a sole with a good grip to prevent
sliding of the shoe. The sole should bend where the toes bend.
Water repellent and
"breathing" characteristies will depending on climate. Since the
swing makes a golf shoe wear upfront, protection against wear and water should
also be built into the front portion of a golf shoe.
-For increased stability in the
swing a slightly concave and relatively wide sole, as well as a stable heel cup
is recommended. The sole and heel of the shoe may preferably be made in one
straight piece with continous contact with the ground for better grip instead
of the traditional
2-piece construction. Elevation of
the heel: about 1/2 inch.
-The grip pattern of the sole should
in the front portion prevent sliding sideways and make a good contact with the
ground in the front swing, especially that of the right foot. In the back
portion of the shoe the grip pattern should prevent sideways and forward
sliding for stability of the swing and to prevent falling when walking
downhill.
Metal spikes today undoubtedly give
the best grip in the swing. Soft spikes do not give as good a grip, but we have
probably not seen the end of research on better soft spikes and sole grip-
patterns. Metal spikes, on the other hand, often give other comfort problems.
-For the swing it is important that
pronation is not overcorrected when analysing the walking pattern.
-Specially made orthotics are needed
only if the characteristics of the shoes prove unsatisfactory and if a shoe and
foot analysis show that it is impossible to choose another better fitted-shoe.
Summary of a presentation at the 'Sports
Achievements & Health Conference" held by the Swedish Golf Federation
2001